
Guidance for Injection
PDpoetin® can be injected into your body using two different ways (routes) as described below. Follow your healthcare provider’s instructions about how you should inject PDpoetin®. In patients on hemodialysis, the intravenous (IV) route is recommended.
Before use, leave the PDpoetin® syringe to stand until it reaches room temperature. This usually takes between 15 and 30 minutes. Do not remove the syringe’s needle cover while allowing it to reach room temperature.
Only take one dose of PDpoetin® from each syringe.
PDpoetin® is given alone and not mixed with other liquids for injection.
Do not shake PDpoetin® Prolonged vigorous shaking may damage the product. If the product has been shaken vigorously, don’t use it.
Check the syringe, to make sure it is the right dose, has not passed its expiry date, is not damaged, and the liquid is clear and not frozen.
Choose an injection site. Do not inject PDpoetin® into an area that is tender, red, bruised, hard, or has scars or stretch marks. Recommended sites for injection are:
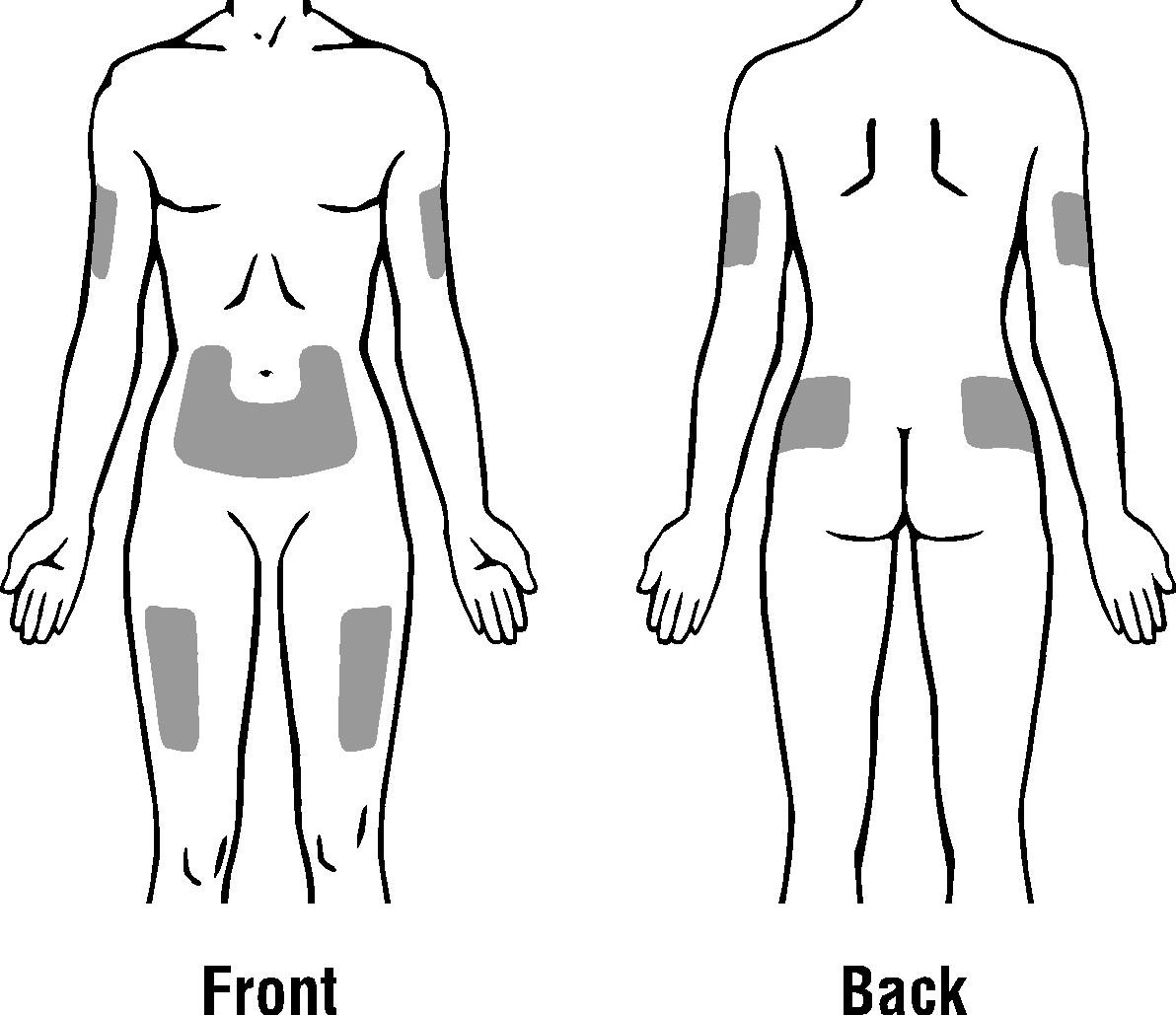
The outer area of the upper arms
The abdomen (except for the 2-inch area around the navel)
The front of the middle thighs
The upper outer area of the buttocks
Subcutaneous Route:
- Wash your hands. Use an antiseptic swab on the injection site, to disinfect it.
- Hold the pre-filled syringe by the body of the syringe with the covered needle pointing upward.
- Do not hold by the plunger head, plunger or needle cover.
- Do not pull back on the plunger at any time.
- Do not remove the needle cover from the pre-filled syringe until you are ready to inject your PDpoetin®.
- Take the cover off the syringe by holding the barrel and pulling the cover off carefully without twisting it. Don’t push the plunger, touch the needle or shake the syringe.
- Pinch a fold of skin between your thumb and index finger. Don’t squeeze it.
- Push the needle in fully. Your doctor or nurse may have shown you how to do this.
- Push the plunger with your thumb as far as it will go to inject the entire amount of liquid. Push it slowly and evenly, keeping the skin fold pinched.
- When the plunger is pushed as far as it will go, take out the needle and let go of the skin.
- When the needle is pulled out of your skin, there may be a little bleeding at the injection site. This is normal. You can press an antiseptic swab over the injection site for a few seconds after the injection.
- Dispose of your used syringe in a safe container.
Intravenous Route:
PDpoetin® can be injected in your vein through a special access port placed by your healthcare provider. This type of PDpoetin® injection is called an intravenous (IV) injection. This route is usually for hemodialysis patients.
- Wipe off the venous port of the hemodialysis tubing with an alcohol wipe.
- Insert the needle of the syringe into the cleaned venous port and pushes the plunger all the way down to inject all the PDpoetin®.
- Remove the syringe from the venous port. Do not recap the needle.
- Dispose of the used syringe and needle.
- Administer over at least one to five minutes, depending on the total dose.
- In hemodialysed patients, a bolus injection may be given during the dialysis session through a suitable venous port in the dialysis line. Alternatively, the injection can be given at the end of the dialysis session via the fistula needle tubing, followed by 10 ml of isotonic saline to rinse the tubing and ensure satisfactory injection of the product into the circulation.
- A slower administration is preferable in patients who react to the treatment with “flu-like” symptoms.
- Do not administer PDpoetin® by intravenous infusion or in conjunction with other drug solutions.